Medicare Advantage Plans...the Pros and Cons for AVRMC’s Long Term Survival

Description: How Medicare Advantage Plans Impact the Survival of Arkansas Valley Regional Medical Center... Complete Brochure in Galley Below...
Medicare Advantage Plans...the Pros and Cons for AVRMC’s Long Term Survival
In 1997, the US Congress passed the legislation that created a new hospital designation called Critical Access Hospital (CAH). This legislation was designed to save rural hospitals from closing by providing additional funds above and beyond submitting claims and being paid for services rendered. Prior to 1997, many rural hospitals had already closed, or significantly scaled back the healthcare services offered or were under threat of closing due to inadequate funding from Centers for Medicare & Medicaid Services (CMS aka Original Medicare), state Medicaid agencies and other insurance payors. Hospitals were able to demonstrate to Congress two very important points.
First, healthcare is local and time sensitive. Local citizens need an Emergency Department and a hospital within 30 minutes to an hour for many healthcare conditions to better ensure an optimal outcome. Secondly, rural hospitals were under the same Medicare/Medicaid Conditions of Participation (CoP), which are the rules and regulations that all hospitals must comply with continuously to be certified to receive funds from CMS, yet they did not have high enough volumes of patients to cover the costs of staffing, facilities, supplies and equipment to remain in compliance with CMS regulations.
In 2017, AVRMC converted from the federal designation called Prospective Payment System (PPS) to the Critical Access Hospital (CAH). In addition to submitting claims and being paid, the CAH designation allowed AVRMC to submit an annual Cost Report to CMS. This Cost Report allows AVRMC, as a CAH, to submit Medicare Allowable Expenses and Medicare Bad Debt for the prior Fiscal Year for the original Medicare beneficiaries that received inpatient, outpatient, and Emergency Department (ED) healthcare services at AVRMC. The Medicare Advantage beneficiaries are not included in this calculation per current regulations. That is a flaw in how CMS developed and deployed the Medicare Advantage (Medicare Part C) program when it was implemented in 2003. The Medicare Advantage plans initially did not get much attention for many years and enrollments remained very low. In the last 3-5 years, the enrollments have skyrocketed, especially in rural areas. Back in 2018, AVRMC received additional funding from CMS related to the Cost Report. With the rapid growth of Medicare Advantage enrollments since 2017, that additional funding has declined from about $1 million annually to about $200K in 2022 and even less for 2023.
Please know that Medicare Advantage plan members can switch back to Original Medicare and have until March 31, 2024 to do so.
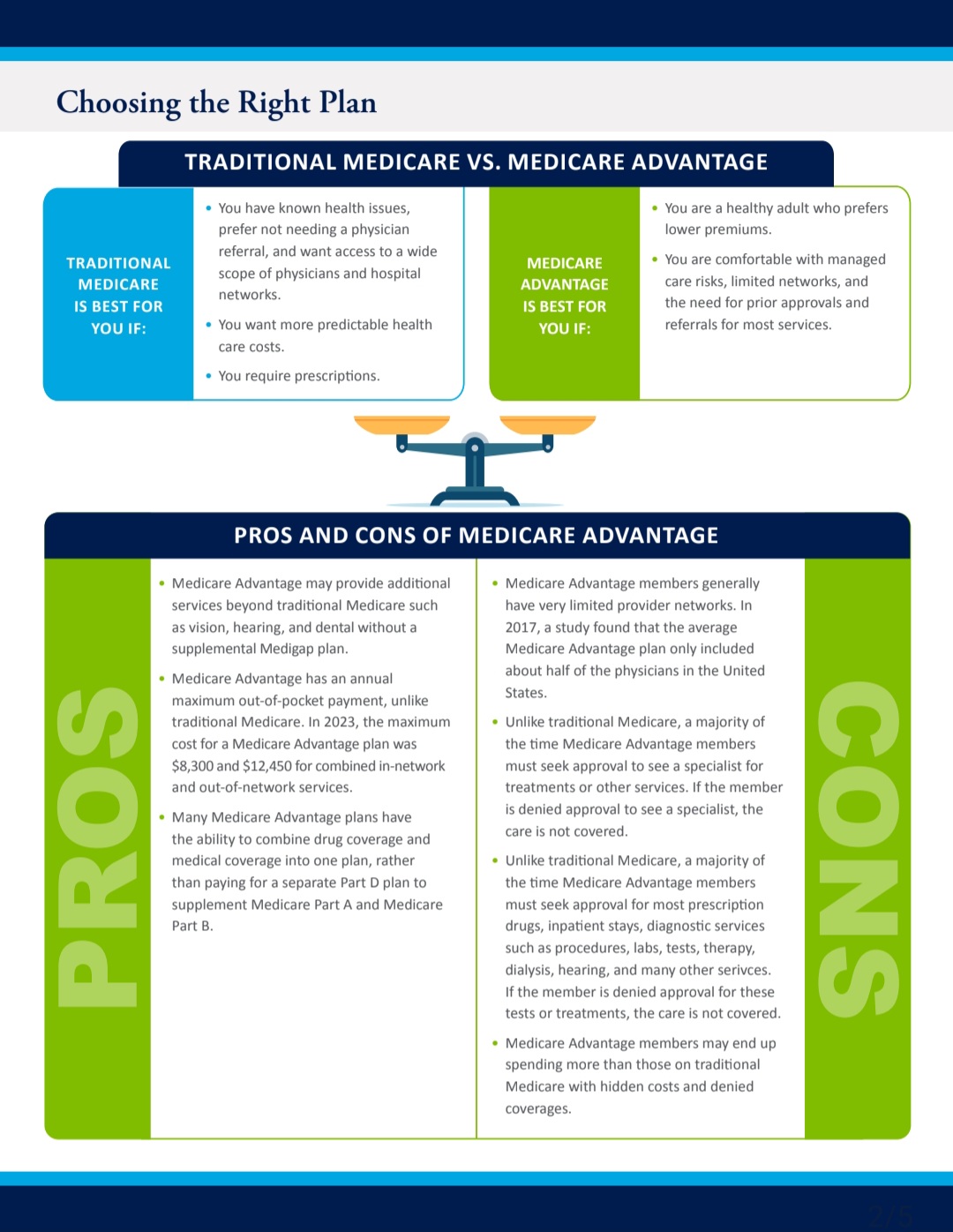
It is highly encouraged that Medicare Advantage plan members switch back to On top of that significant decline in additional CAH funding, Medicare Advantage plans are not conducting themselves in an ethical business way.
They consistently deny claims for Inpatient, ED, and Outpatient services even when AVRMC has an authorization for the services rendered. Additionally, AVRMC is slow paid or underpaid per the contract terms and fee schedule with the Medicare Advantage plans like Humana, UnitedHealthcare and Cigna for example. Another problem for Medicare Advantage plan members is they begin to realize the limitations of their plan when they use the ED or are admitted as an inpatient or observation patient. The wait for authorizations is very long. However, when they are very sick, and a patient in the hospital they can’t switch back to original Medicare until the annual Open Enrollment period.
Then when their health improves and they can be discharged to a lower level of care, they now learn that most Skilled Nursing Facilities, Home Health Agencies, Outpatient PT/OT, Respiratory and other ancillary services do not contract with Medicare Advantage plans or cap the maximum number of Medicare Advantage enrollees they will accept, and the closest facilities are in Pueblo and Colorado Springs. This puts a significant burden on the patient, their families, and support networks.
There are aspects of the Medicare Advantage (MA) plans that make them very appealing to original Medicare beneficiaries such as the monthly cash card they can use on most any expense. Where did the MA plans get the extra funding for the cash card you might ask? From the CAH Medicare Cost Report funds initially intended for rural hospitals.
AVRMC is in the process of trying to renegotiate our contracts with the Medicare Advantage plans starting with Humana since they have the bulk of members in our area. This contract was signed back in 2011 and is long overdue for an improvement in the contract terms. This includes terms such as the timely filing of medical claims deadline which is 90 days, and the fee schedule rates to be increased by 30-40% to account for the loss of Critical Access Hospital Medicare Cost Report additional funding for rural hospitals.
Thank you for choosing AVRMC, your Critical Access Hospital, for your healthcare needs.
AVRMC is a Founding Advertising Contributor on SECO News...
Follow SECO News on Facebook.
Subscribe to the SECO News YouTube Channel.
Click to Zoom


Healthcare Sponsor

.jpg)
.png)



.png)




 (728 x 90 px).png)














